Surgery of the Eyelid and Eyebrow

Voted Best of Berks—
eight years in a row!
Upper Lid Blepharoplasty
Rejuvenation of the Upper Face
When you look at a person, your attention is drawn to their face and particularly their eyes. A person's eyelids, brows and cheeks are designed to convey emotions. Your face can appear either tired or energetic and youthful. Blepharoplasty is intended to produce a more vibrant appearance.
 |
 |
| Before | After upper lid blepharoplasty |
 |
 |
| Before | After upper lid blepharoplasty |
Upper lid blepharoplasty surgery (also known as an "eyelid tuck") reduces the fold of eyelid skin and fat that covers the skin above the eyelashes. The visible skin between your eyelashes and eyelid crease is called the "eye shadow space." In females, make-up or eye shadow is normally applied in this area. A high eye shadow space is desirable. The height of the eye shadow space is determined by the height of the lid crease and how much excess skin and fat hang over the crease. Blepharoplasty forms a distinct crease and reduces the excess skin and fat, producing a pleasing eye shadow space.
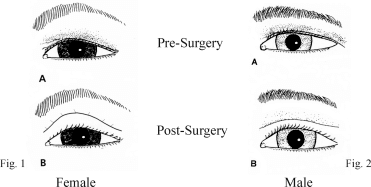
Men also benefit from eyelid surgery. Most males do not desire a high eye shadow space, wanting to appear more masculine. However, a small visible area of smooth skin above the lashes is necessary to convey a youthful appearance. This can be achieved with a blepharoplasty.
 |
 |
| Before | After upper lid blepharoplasty |
 |
 |
| Before | After upper lid blepharoplasty |
 |
 |
| Before | After bilateral upper lid blepharoplasty |
The goal of upper lid blepharoplasty is not to simply remove excess skin but to reshape the lid. If more skin is removed than necessary the eyebrows can be pulled downwards. More importantly, if too much skin is removed, difficulty closing the eyes and dryness of the eyes can occur.
As an ophthalmologist, the health of your eyes is the most important factor in planning surgery. Prior to surgery, Dr. Goldberg will evaluate the lubrication of your eyes to ensure that your eyes will be comfortable after surgery. In some cases, treatment of pre-existing dry eyes will be necessary before undergoing eyelid surgery.
Many patients with excess skin and fat in the upper lids also have true eyelid ptosis. In patients with ptosis, the whole eyelid drops, covering part of the pupil. Ptosis should be corrected by tightening the eyelid lifting muscle. Raising the upper lid can be performed at the time of blepharoplasty. Ptosis repair requires extensive experience and is usually performed by an ophthalmologist who specializes in eyelid surgery.
 |
 |
| Before | After upper lid ptosis repair and blepharoplasty |
 |
 |
| Before | After upper lid ptosis repair and blepharoplasty |
The position and fullness of the brows is an important consideration in planning upper lid blepharoplasty. Some patients have thick, heavy brows. In these patients, a browplasty can be performed at the same time as upper lid blepharoplasty to reduce unwanted brow thickness.
Many patients who desire a blepharoplasty also have deflation of the brow fat. In young adults, the brow is full and shaped by the fat under the brow. With age, the fat beneath the skin atrophies. The brows then become wrinkled and deflated. At the time of upper lid blepharoplasty, the outside part of the incision can be angled upwards to support the deflated brow. This produces a more youthful, energetic appearance.
The muscles between the eyebrows (Glabellar muscles) produce frown lines or vertical folds between the brows. The muscles also pull down the inner brow. During blepharoplasty, these Glabellar muscles can be removed to smooth the area between the eyebrows. If the wrinkles are deep, a procedure can be performed to undermine and flatten the wrinkles through tiny, self-healing incisions.
There is some risk of localized numbness after the glabellar smoothing procedure. This numbness usually resolves with time. In addition, there is always some residual muscle activity after this procedure which can be improved by Botox injections to this area.
Brow Lift
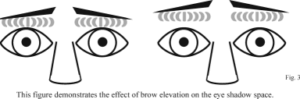
The eyebrows are the "curtain rods" of the eyelids. By raising and lowering your brows you can change the amount of visible "eye shadow space." Lowering the brows increases the amount of redundant skin which hangs down below the lid crease and covers the eye shadow space. Therefore, it is important to address the brows when considering an upper lid blepharoplasty. If a person has loose brows removing eyelid skin will simply pull the eyebrows downwards. In addition, raising the brows helps create a friendlier appearance. During a coronal brow lift the forehead is also smoothed.
There are essentially five techniques to address brow laxity. You can discuss with your surgeon which techniques are right for you.
Coronal Brow Lift - In a coronal brow lift, an incision is made behind the hairline. Excess scalp is removed to elevate the brows. In addition, the forehead is smoothed. The surgeon partially removes the muscles which lower the brow. These muscles are located between the eyebrows and produce the vertical furrows, called glabellar folds. Besides raising the brows, removing these muscles reduces these glabellar folds. The hair is not shaved during the procedure.
The Coronal Brow Lift can also be performed endoscopically, with small instruments placed through small incisions behind the hair line. The glabellar folds are treated. Then the forehead and eyebrows are pulled back. Brow elevation may not be as complete and last as long after endoscopic surgery as with a full-incision coronal approach.
Because the nerves which supply feeling to the forehead run through the brows, patients will notice numbness of the forehead and scalp after surgery. This numbness improves with time.
Brow lifting may also stretch or damage the nerve that directs movement of the brow. Damage to this motor nerve will produce a brow palsy, or immobile brow. The palsy is usually temporary but may be permanent in some cases.
A coronal or endoscopic brow lift does raise the hairline. This is usually not a problem in females. However, it does prevent the use of this procedure in many males unless the incision is placed in front of the hairline.
Lateral hairline subcutaneous brow lift - A lateral hairline subcutaneous brow lift is, in essence, a mini-coronal lift. The incisions are placed in the hairline but do not extend to the central forehead. Excess forehead skin is removed to elevate the brows. The lateral hairline subcutaneous brow lift effectively elevates and shapes the outer brow. The procedure is usually performed on patients with lateral brow ptosis who either don't require a coronal brow lift or don't want to undergo a full coronal lift. The recovery is quicker after a lateral hairline subcutaneous brow lift than after a coronal brow lift.
The lateral hairline subcutaneous brow lift does produce a scar, but the scar is hidden at the hairline. The procedure does not raise the hairline and, in fact, tends to pull the hair down at the corners of the hairline. This effect is desirable in those with hair loss at the corners of the hairline.
The lateral subcutaneous hairline brow lift does not reduce glabellar lines. However, the procedure can be combined with removal of the glabellar muscles through the blepharoplasty incision. Some patients do develop numbness of the lateral forehead and scalp after surgery, but in almost all cases the numbness resolves with time. Brow palsy is a concern, as with a coronal brow lift.
Direct Brow Lift - A direct brow lift is performed by excising skin just above the brow, or between deep forehead wrinkles, fixating the brows at a higher position. This procedure does not raise the hairline and is usually performed in males. While the most effective procedure to elevate the brows, a direct brow lift leaves a visible scar.
 |
 |
| Before | After later direct brow lifting, upper lid blepharoplasty and ptosis repair |
 |
 |
| Before | After later direct brow lifting, upper lid blepharoplasty and ptosis repair |
Lateral direct brow lift - A lateral direct brow lift is performed by excising a small amount of skin between the lateral brow and the hairline. This procedure is usually performed on older patients with lateral hooding. In some cases, this lateral hooding cannot be treated with blepharoplasty. Instead, brow lifting is required in order to shape and elevate the lateral brow. While a scar is produced, the scar is small and not usually cosmetically apparent in the older patient.
Internal browpexy - The brow can be supported internally through the upper lid blepharoplasty incision. Suture fixation can be used, but is not usually effective. An endotine fixation device can be placed at the time of blepharoplasty. The endotine device fixates the brow in a higher position. The device can often be felt after surgery and so is not used in those patients with thin tissue. The device does dissolve after several months, but produces long-lasting brow elevation.
Lower Lid Blepharoplasty
When you look at a person, your attention is drawn to their face and particularly their eyes. A person's eyelids, brows and cheeks are designed to convey emotions. Your face can appear either tired or energetic and youthful. Blepharoplasty is intended to produce a more vibrant appearance.
Lower lid blepharoplasty is used to reduce the puffiness and extra skin folds in the lower lids and mid-face, producing a more energetic, youthful appearance.
 |
 |
| Before | After lower lid blepharoplasty |
 |
 |
| Before | Before |
 |
|
| After upper and lower lid blepharoplasty | |
 |
 |
| Before | After upper & lower lid blepharoplasty |
 |
 |
| Before | After upper & lower lid blepharoplasty |
Aging causes several changes in the lower lids and mid-face. Fat pads protrude producing lower lid puffiness. Both fine and hard wrinkles appear in the lower lids. In addition, the soft-tissues of the cheek atrophy producing a tear trough deformity below the eyelid.
During a lower lid blepharoplasty, the protruding fatty tissue is removed. The loose eyelid skin may also be redraped and trimmed in order to smooth the lower lid. A hidden incision is made on the inside of the lid in order to remove excess fat. If excess skin is present, the extra skin is removed with a small incision at the outer corner of the eyelids. If skin is removed, the eyelid must be tightened in order to prevent the lower lid from pulling down and rounding.
As an ophthalmologist, the health of your eyes is our main concern. Ophthalmologists have extensive experience working with the complex anatomy of the lower lid fat pads and outer corner of the eyes. An ophthalmologist is also concerned with preventing any eyelid malposition which might affect the long-term health of your eyes.
The incision at the outside corner of the eye is constructed to blend with the laugh lines. The incision line can be red for several months, but will fade with time. While red, the incision can be covered with make-up.
Lower lid blepharoplasty does not eliminate fine lower lid wrinkles. At the time of lower lid blepharoplasty, an eyelid or facial moderate depth peel can be performed to improve fine wrinkles and pigmentation.
Crows feet are wrinkles on the outer corners of the eyes. Crows feet are best addressed with Botox injections which are performed easily in the office.
Fat Injection
Many people also have hollowing below the lids causing the tear trough deformity. In addition, the cheek fat is lost with age. This loss of cheek fat flattens the cheek particularly below the eye and in the area of the cheekbone. This loss of cheek fat is particularly noticeable in those who never had prominent cheek bones. Fat from elsewhere in your body can be injected to replace the fat loss that comes with age. The fat is injected through small incisions and can be used to fill the tear trough and produce a more cosmetically desirable mid-facial contour.
Malar Bags
Malar bags occur in some patients. The bags, situated over the cheekbones, are unsightly and produce an aged and tired appearance. At the time of lower lid blepharoplasty, the bags are redraped and debulked through an extension of the skin incision at the outer corner of the eyelids.
Commonly Asked Questions
1. Will insurance pay for these procedures?
Health Insurance companies will reimburse procedures which are functionally necessary. If the skin of the upper lid actually interferes with your vision, upper lid blepharoplasty may be reimbursed. In order to obtain insurance reimbursement, we must submit photos and visual fields documenting interference with visual function for preauthorization prior to surgery.
Medicare does not preauthorize surgery. Medicare eligibility is determined by a test of your side vision (visual fields) to determine if the upper lid abnormalities are visually significant.
Lower lid blepharoplasty is not usually covered by insurance.
2. What is recovery like?
During the first two days after surgery your eyelids will be swollen. Use cold compresses as much as possible and keep your head elevated on at least two pillows for the first two days. Swelling is more prominent in men with thick skin, particularly those men who undergo both upper and lower lid blepharoplasty.
After the first two days, the swelling begins to improve. By two weeks after surgery most patients only have minor swelling and bruising. However, some thickening of the tissue can persist for weeks. Combining upper and lower lid blepharoplasty will increase the swelling and prolong your recovery period by a few days.
Your vision will also be blurry for several days after surgery due to eyelid swelling. You will not blink normally after surgery and the tear film over your eyes will not be smooth. Although able to function around the home, most patients cannot see well enough to drive for about one week after surgery. Most patients take one to two weeks off from work.
After upper lid surgery, your eyes may feel dry because you will not be able to blink normally. You will be instructed to use ointment to lubricate your eyes for the first week after surgery. Some patients may require lubricating drops or ointment for a longer period.
Please, no yard work or hot tubs for two weeks after surgery to prevent infection.
Avoid strenuous activity, exercise and trauma for two weeks after surgery to prevent damage to the incisions.
3. Are there risks and complications associated with these procedures?
Yes, all surgery has risks. Results are not guaranteed. The following is not a complete list of possible complications.
Eye lid surgery can result in asymmetry, bruising, infection, undesirable scarring, excess residual skin, rounding of the lower lid and the need for additional procedures.
The upper lids will be tight after surgery causing difficulty blinking normally. Your eyes may become dry requiring the use of lubricating drops or ointments. Revision may be necessary.
In rare cases, excess bleeding can result in visual loss or even blindness.
Not every condition is listed. Consult Dr. Goldberg or Dr. Lippe if you have any questions about a condition not described here.
Fig. 1 and Fig. 2 from Eyelid Surgery; Principals and Techniques by Clinton McCord, Jr., M.D., published 1995 by Lippincott-Raven. Used by permission.
Find a Doctor
Physician information including education, training, practice location and more.
Schedule an Appointment
Call 800-762-7132 or make an appointment online.




